Via Scoop.it – Virology News

THERE. IS. NO. YELLOW. FEVER. IN. SOUTH. AFRICA.
WHO does NOT think so – and there is a map to prove it.
Via Scoop.it – Virology News
THERE. IS. NO. YELLOW. FEVER. IN. SOUTH. AFRICA.
WHO does NOT think so – and there is a map to prove it.
Via Scoop.it – Virology News
Yellow fever is endemic not only in South Africa, but also in 33 other countries of the continent with a combined population of 508 million. …, Srikanth Radhakrishna…
THERE. IS. NO. YELLOW. FEVER. IN. SOUTH. AFRICA.
Are we clear on this? Unless it is imported from another country – because it is assuredly NOT endemic!! And irresponsible statements like this do not help anyone – except certain vaccine clinics.
My participation in an acrimonious exchange in the Comments section of a recent article in The Scientist by UCT’s own Nicoli Nattrass has brought something home to me that I had hoped was long dead. That is, that there are some apparently quite well-educated people who still believe that HIV either does not actually exist, or that it does not cause Acquired Immune Deficiency Syndrome (AIDS).
I find this almost unbelievable: that people in this day and age can make statements like
boggles my mind. There are 236 870 papers at least in the scientific literature since the early 1980s on HIV: are we to understand that probably over a million authors from al over the world have willingly participated in a fraud that has to be the biggest ever perpetrated? Or do we believe that there is something called HIV, that it causes AIDS, and that the overwhelming proportion of the world’s scientists have no problem with this?
I know what I think – and I am going to reprise it here. I put this together in 2001 or thereabouts; however, nothing has changed. HIV still exists, it still causes AIDS, and anyone who denies this is truly, truly invincibly ignorant.
Human Immunodeficiency Virus (HIV) is a typical retrovirus of the genus Lentivirus, family Retroviridae: these are viruses which have single-stranded RNA as their genetic material, but multiply via a double-stranded DNA intermediate. The replication and classification of such viruses is discussed in greater detail on this site, as well as at the Leicester site.
The virus infects its target cells – which happen to mainly be helper T-lymphocytes, because these are the cells which have the highest density of the preferred receptor molecule – by specifically attaching to a protein carried on the surface of the cells known as CD4. This is shown here. An animated view of the whole infection process is shown here; a more detailed schematic animated view here. The process is discussed in detail here; however, what happens is that virus particles fuse with the target cells, and deliver their genetic material plus inside. This RNA is then converted into DNA by means of a unique viral enzyme called reverse transcriptase. The double-stranded DNA is then inserted randomly into a host cell chromosome by means of another viral enzyme (integrase). As part of the host chromosome it is expressed exactly the same way as host DNA – AND IS NOW PART OF THE CELL AND CANNOT BE REMOVED. This means that infected cells are infected for life, which is different to most other types of virus infections: cells harbouring viral DNA continue to make infectious virus particles until they die or are killed.

SEE HERE FOR GRAPHICAL REPRESENTATION OF THE CELLULAR INFECTION PROCESS (Courtesy Russell Kightley)

“An HIV-infected person is diagnosed with AIDS when his or her immune system is seriously compromised and manifestations of HIV infection are severe.
“The U.S. Centers for Disease Control and Prevention (CDC) currently defines AIDS in an adult or adolescent age 13 years or older as the presence of one of 26 conditions indicative of severe immunosuppression associated with HIV infection, such as Pneumocystis carinii pneumonia (PCP), a condition extraordinarily rare in people without HIV infection. Most other AIDS-defining conditions are also “opportunistic infections” which rarely cause harm in healthy individuals.
A diagnosis of AIDS also is given to HIV-infected individuals when their CD4+ T-cell count falls below 200 cells/cubic millimeter (mm3) of blood.
Healthy adults usually have CD4+ T-cell counts of 600-1,500/mm3 of blood. In HIV-infected children younger than 13 years, the CDC definition of AIDS is similar to that in adolescents and adults, except for the addition of certain infections commonly seen in pediatric patients with HIV. (CDC. MMWR 1992;41(RR-17):1; CDC. MMWR 1994;43(RR-12):1).
In many developing countries, where diagnostic facilities may be minimal, healthcare workers use a World Health Organization (WHO) AIDS case definition based on the presence of clinical signs associated with immune deficiency and the exclusion of other known causes of immunosuppression, such as cancer or malnutrition.
An expanded WHO AIDS case definition, with a broader spectrum of clinical manifestations of HIV infection, is employed in settings where HIV antibody tests are available (WHO. Wkly Epidemiol Rec. 1994;69:273).”
There is very little doubt among the vast majority of people working with HIV or with people with AIDS, that HIV causes AIDS (see above). The media tended to present everything in terms of a two-sided debate, with equal credence being given to both “sides”. This is very misleading for the population at large, as they are presented with two sets of information that receive equal billing – and they are not qualified to judge between the viewpoints.
Quite simply, there is a vast body of evidence supporting the proposition that HIV causes AIDS.
I have presented some of the most compelling below; there is an enormous body of other evidence available on the Web, let alone in medical libraries. The same cannot be said for the alternative view(s). Perhaps the “best” of the denialist sites is is probably the “Rethinking AIDS” site. This has a wealth of (dis)information on the subject, including such gems as the following, from Kary Mullis:
“If there is evidence that HIV causes AIDS, there should be scientific documents which either singly or collectively demonstrate that fact, at least with a high probability. There is no such document.” (Sunday Times London, 28 nov. 1993).
That this statement is nonsense is amply demonstrated by the following:
“The evidence that AIDS is caused by HIV-1 or HIV-2 is clear-cut, exhaustive and unambiguous. This evidence meets the highest standards of science. The data fulfill exactly the same criteria as for other viral diseases, such as poliomyelitis, measles and smallpox:
- Patients with acquired immune deficiency syndrome, regardless of where they live, are infected with HIV.
- If not treated, most people with HIV infection show signs of AIDS within 5-10 years. HIV infection is identified in blood by detecting antibodies, gene sequences or viral isolation. These tests are as reliable as any used for detecting other virus infections.
- Persons who received HIV-contaminated blood or blood products develop AIDS, whereas those who received untainted or screened blood do not.
- Most children who develop AIDS are born to HIV-infected mothers. The higher the viral load in the mother the greater the risk of the child becoming infected.
- In the laboratory HIV infects the exact type of white blood cell (CD4 lymphocytes) that becomes depleted in persons with AIDS.
- Drugs that block HIV replication in the test tube also reduce viral load and delay progression to AIDS. Where available, treatment has reduced AIDS mortality by more than 80%.
- Monkeys inoculated with cloned SIV DNA become infected and develop AIDS.
Further compelling data are available. HIV causes AIDS. It is unfortunate that a few vocal people continue to deny the evidence. This position will cost countless lives.”
AIDS and HIV infection are invariably linked in time, place and population group.
Historically, the occurence of AIDS in human populations around the world has closely followed the appearance of HIV. In the United States, the first cases of AIDS were reported in 1981 among homosexual men in New York and California, and retrospective examination of frozen blood samples from a U.S. cohort of gay men showed the presence of HIV antibodies as early as 1978, but not before then. Subsequently, in every region, country and city where AIDS has appeared, evidence of HIV infection has preceded AIDS by just a few years (CDC. MMWR 1981;30:250; CDC. MMWR 1981;30:305; Jaffe et al. Ann Intern Med 1985;103:210; U.S. Census Bureau; UNAIDS).
Many studies agree that only a single factor, HIV, predicts whether a person will develop AIDS.
Other viral infections, bacterial infections, sexual behavior patterns and drug abuse patterns do not predict who develops AIDS. Individuals from diverse backgrounds, including heterosexual men and women, homosexual men and women, hemophiliacs, sexual partners of hemophiliacs and transfusion recipients, injection-drug users and infants have all developed AIDS, with the only common denominator being their infection with HIV (NIAID, 1995).
In cohort studies, severe immunosuppression and AIDS-defining illnesses occur almost exclusively in individuals who are HIV-infected.
For example, analysis of data from more than 8,000 participants in the Multicenter AIDS Cohort Study (MACS) and the Women’s Interagency HIV Study (WIHS) demonstrated that participants who were HIV-seropositive were 1,100 times more likely to develop an AIDS-associated illness than those who were HIV-seronegative. These overwhelming odds provide a clarity of association that is unusual in medical research (MACS and WIHS Principal Investigators, 2000).
In developing countries, patterns of both rare and endemic diseases have changed dramatically as HIV has spread, with a far greater toll now being exacted among the young and middle-aged, including well-educated members of the middle class.
In developing countries, the emergence of the HIV epidemic has dramatically changed patterns of disease in affected communities. As in developed countries, previously rare, “opportunistic” diseases such as PCP and certain forms of meningitis have become more commonplace. In addition, as HIV seroprevalence rates have risen, there have been significant increases in the burden of endemic conditions such as tuberculosis (TB), particularly among young people. For example, as HIV seroprevalence increased sharply in Blantyre, Malawi from 1986 to 1995, tuberculosis admissions at the city’s main hospital rose more than 400 percent, with the largest increase in cases among children and young adults. In the rural Hlabisa District of South Africa, admissions to tuberculosis wards increased 360 percent from 1992 to 1998, concomitant with a steep rise in HIV seroprevalence. High rates of mortality due to endemic conditions such as TB, diarrheal diseases and wasting syndromes, formerly confined to the elderly and malnourished, are now common among HIV-infected young and middle-aged people in many developing countries (UNAIDS, 2000; Harries et al. Int J Tuberc Lung Dis 1997;1:346; Floyd et al. JAMA 1999;282:1087).
HIV can be detected in virtually everyone with AIDS.
Sensitive testing methods, including the polymerase chain reaction (PCR) and improved culture techniques, have enabled researchers to find HIV in patients with AIDS with few exceptions. HIV has been repeatedly isolated from the blood, semen and vaginal secretions of patients with AIDS, findings consistent with the epidemiologic data demonstrating AIDS transmission via sexual activity and contact with infected blood (Bartlett, 1999; Hammer et al. J Clin Microbiol 1993;31:2557; Jackson et al. J Clin Microbiol 1990;28:16).
Via Scoop.it – Virology News
Meta-analyses of the few studies providing effects with adjustment for confounders suggest that in high-risk populations, oral oseltamivir may reduce mortality (odds ratio, 0.23 [95% CI, 0.13 to 0.43]; low-quality evidence), hospitalization (odds ratio, 0.75 [CI, 0.66 to 0.89]; low-quality evidence), and duration of symptoms (33 hours [CI, 21 to 45 hours]; very low–quality evidence) compared with no treatment. Earlier treatment with oseltamivir was generally associated with better outcomes. Inhaled zanamivir may lead to shorter symptom duration (23 hours [CI, 17 to 28 hours]; moderate-quality evidence) and fewer hospitalizations (odds ratio, 0.66 [CI, 0.37 to 1.18]) but more complications than no treatment. Direct comparison of oral oseltamivir and inhaled zanamivir suggests no important differences in key outcomes. Data from 1 study suggests that oral amantadine may reduce mortality and pneumonia associated with influenza A. No included study evaluated rimantadine. Image courtesy of Russell Kightley Media
Via www.annals.org
Via Scoop.it – Virology News
Although in its sixth year of publication, this year’s barometer is the first to include data on early infant HIV testing for babies born to HIV-positive mothers and shows that about half of all babies born to HIV-positive mothers are now being tested for the virus at six weeks of age, an important step to ensuring they access the early HIV treatment recommended for all children younger than one under national guidelines. In 2009, only about a quarter of such babies were being tested using the sensitive polymerase chain reaction – tests that confirm whether HIV-exposed infants are HIV-positive. The report also found that almost all pregnant women are now tested for HIV, which has helped lower mother-to-child HIV transmission to below 4 percent in the country.
Via allafrica.com
Via Scoop.it – Virology News
FRANCISTOWN: Poor knowledge about HIV/Aids and other sexually transmitted diseases among young people has compelled a Gaborone-based youth to create a group on the popular social network, Facebook, to enlighten his peers about the scourge. Ex Africa, semper aliquid novi. Or a Facebook page, in this case.
Via www.mmegi.bw
Via Scoop.it – Virology News
Scientists from the US Centers for Disease Control and Prevention (CDC) have discovered evidence of a new influenza type A virus in Guatemalan fruit bats. “…for reassortment to occur, the bat flu virus would have to be capable of infecting a different animal, such as a pig, horse or dog, at the same time as a human flu virus. So far, the bat flu virus has only been found in little yellow-shouldered bats. These fruit bats are not native to the US, but quite common in Central and South America. The bats don’t bite people, but it is feasible they could shed the virus onto foods like fruit and vegetables that are then eaten by humans and other animals.” And if you watched “Contagion”, you will rmember the bulldozer knocking down the tree, which disturbed the bat, which roosted in a pigpen, where pigs ate the faeces, and – recombination occurred!
Via www.medicalnewstoday.com
Via Scoop.it – Virology News
Tinderbox: How the West Sparked the AIDS Epidemic and How the World Can Finally Overcome It, attempts to pinpoint the birth and early life of HIV and AIDS. Considering a wealth of evidence, the authors suggest that the European Scramble for Africa during the late 19th and early 20th century helped turn localised outbreaks of the infection into a global epidemic.
Read more: http://www.dailymail.co.uk/health/article-2107605/HIV-epidemic-driven-colonialism-Africa-century-ago.html#ixzz1nhlAqwEM
Via www.dailymail.co.uk
Via Scoop.it – Virology News
My family and I just watched “Contagion” on pay TV – and were most impressed. Reasonably true to life, all sorts of realistic scenarios, Ian Lipkin appearing as an extra – and one wonderful quote: “Someone doesn’t have to weaponise the bird flu. The birds are doing that”. Contagion is only a movie – but that’s so true. Oh, and an uncredited appearance by Darren Martin’s wonderful recombination analysis package, RDP 2.0 – at 1hr 15 min from the end.
While curating Virology News today, I came across another reprocessing of new that I had come across earlier concerning apparent natural protection of some African female sex workers against HIV infection: this was the intriguingly-entitled “African women’s genitals provide clue to HIV prevention“, in what appears to be an online Nigerian newspaper.
This recapitulates, very accurately, the information I reported in Virology News, which was the subject of a news release following the publication in the September 2011 edition of PLoS One of a study entitled “High Level of Soluble HLA-G in the Female Genital Tract of Beninese Commercial Sex Workers Is Associated with HIV-1 Infection”. The gist of this is that:
“HIV-resistant sex workers in Africa have a weak inflammatory response in their vaginas – a surprise for the researchers, who were expecting the contrary considering the women’s high exposure to the virus.”
This may lend further credence to the observation that progression to AIDS in HIV-infected people is associated with a state of chronic immune activation – and that SIV-infected vervet monkeys do not exhibit such chromic immune activation, and do not progress like humans do.
What is interesting about the Nigerian article, however, is not what it reports – it is the online comments that follow it. Here is a selection:
“Was HIV realy discovered in Africa ? Forget the western media propaganda . I have believed , for years , that HIV is a laboratory virus designed for genocide in the thick of apartheid inhuman policies in South Africa .”
“Neither did HIV originate nor was it perculiar to Africa. It was the creation of the Western countries to stsyematically reduce African population. that the subjects of this study were exposed to HIV virus attests to this fact.”
And my personal favourite:
“So you have already swallowed up the white propaganda that the AIDS virus was first discovered in 1981 in a remote area of central Africa in the green monkey! A fairy tale, which never explains why prior to its first clinical detection among western homosexual men in the late seventies, no case was found in Africans, and no animal or human population died off in Africa, yet the homosexual population of the west was seriously threatened until their protected sex campaign took off.
You must be unaware that about 35 years ago the Soviet KGB told the world the truth about AIDS….
Jakob Segal, a former biology professor at Humboldt University in then-East Germany, proposed that HIV was engineered at a U.S. military laboratory at Fort Detrick, by splicing together two other viruses, Visna and HTLV-1. According to his theory, the new virus, created between 1977 and 1978, was tested on prison inmates who had volunteered for the experiment in exchange for early release. He further suggested that it was through these prisoners, most of who were homosexuals, that the virus was spread to the population at large.”
What is depressing is that there is just one comment saying “…where HIV started is of little significance now. the issue is that our brothers Africans are the ones affected so we must work hard to find the cure and save our brothers.”
What is obvious is that, even in an environment such as one of the most developed nations in Africa, where intelligent science reporting is happening, the public seems to be alarmingly misinformed about the origin of HIV and predisposed to believe racist conspiracy theories that were debunked years ago.
FACT:
HIV did not come from “green monkeys” and was not discovered in 1981: the virus was described in 1983 and 1984, and HIV entered the human population in central Africa multiple times, from chimpanzees and possibly also from gorillas, almost certainly via bushmeat – and this happened in the 1930s or even earlier.
FACT:
HIV could not possibly have resulted from the splicing together of Visna virus and HTLV-1, as no HIV sequence bears any strong resemblance to either virus – and especially not to both of them in different parts of their genomes, as they would be expected to if they were artificial recombinants. Moreover, the first HIV that has been reliably dated comes from a sample taken in the Congo in 1959.
All of these facts can be easily discovered by a trawl of either the scientific literature, or a first-level digest of that literature by reputable journalists. All else is fiction…and malicious fiction at that, whether or not such supposed luminaries as Thabo Mbeki believe it.
ANOTHER note added in response to Timothy Julian, below, who seems not to understand anything about retrovirus and especially lentivirus evolution. Here is an unrooted radial relationship diagram (aka “phylogenetic” diagram) depicting whole genome sequence relationships between HIV-1, HIV-2, 2 SIVs, Maedi-Visna ad bovine leukaemia viruses, feline and bovine immunodeficiency and human and simian T-cell lymphotropic viruses. Done by me today from Genbank sequences, using CLC Genomics Workbench ver 7.
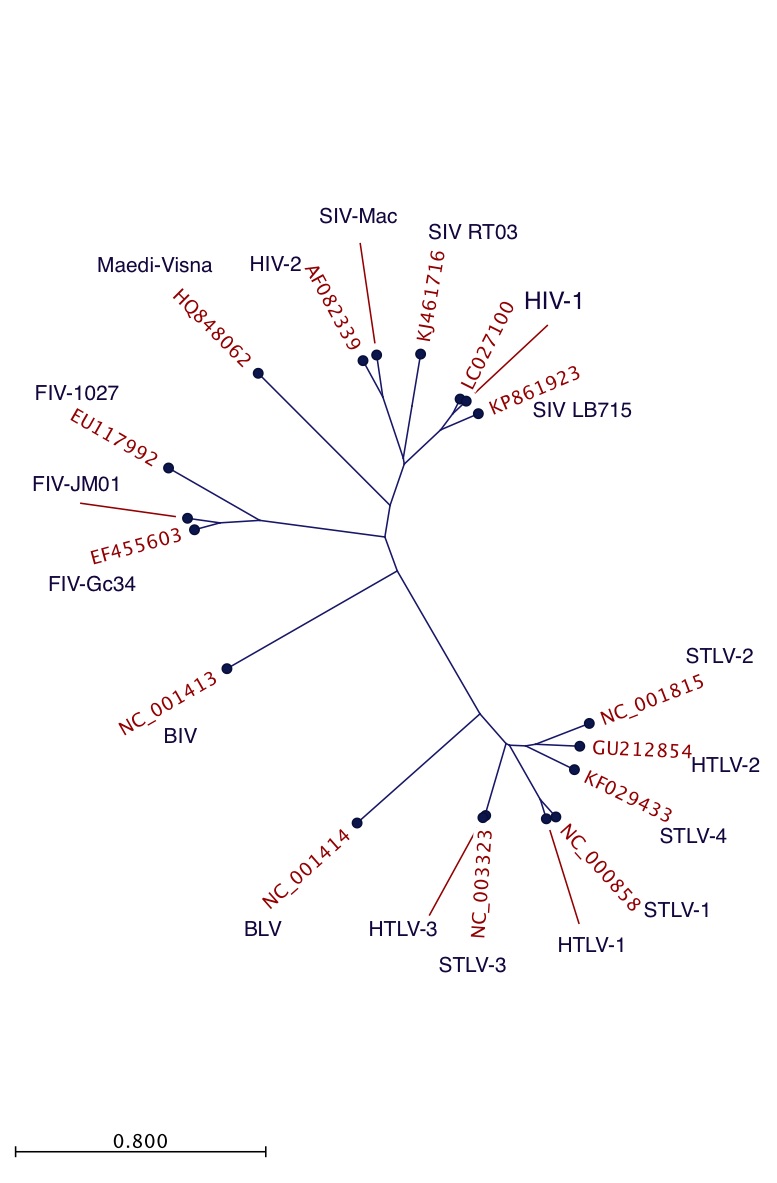
Radial tree for retrovirus complete genome sequences
What it shows is that:
If HIV-1 derives from artificial constructs derived from FIVs, which are less closely related to them than is MVV, then is the same true for the whole primate cluster? Really? When it is pretty obvious that they are (a) evolutionarily related most closely to one another, (b) evolutionarily diverged to quite a considerable extent? So were they all made individually?? Then cleverly given to different bush-dwelling primates in Africa? How desperately unlikely is that?? You appear not to have heard of teh principle of parsimony, which is that the simplest explanation that covers all of the facts is probably correct – which in this case, is that both HIVs and all of the SIVs have a common evolutionary origin, thousands of years ago – and that all lentiviruses also have a common origin, millions of years ago.
Seriously, Timothy: give it a rest. You know less than Jon Snow.






{kind=link}
{kind=link}
{kind=link}
{kind=link}